An abdominal aortic aneurysm (AAA) is the local expansion of the abdominal aorta, a large artery that takes blood from the heart to the abdomen and lower parts of the body. It is a condition that tends not to produce symptoms until it ruptures. An aneurysm can rupture without warning, causing sudden collapse or death of the patient. Most abdominal aortic aneurysms occur below the kidneys (i.e., are infra-renal).
A ruptured AAA requires emergency surgery. Screening and intervening to treat larger AAAs reduces the risk of rupture, and the National Abdominal Aortic Aneurysm Screening Program (NAAASP) was introduced in 2010 to identify and treat at-risk aneurysms prior to rupture. Once detected, treatment to repair the AAA before it ruptures can be planned with the patient, and surgery is typically performed as an elective procedure.
Aneurysms may be treated by either open surgery, or by an endovascular repair (EVAR). In open surgery, the AAA is repaired through an incision in the abdomen. An EVAR procedure involves the insertion of a stent graft through the groin. Both are major operations. The risk of death after elective AAA surgery is roughly 4% for open surgery and 1% following endovascular repair. The decision on whether EVAR is preferred over an open repair is made jointly by the patient and the clinical team, taking into account characteristics of the aneurysm, patient age, and fitness.
As people age, they can suffer from the narrowing of the carotid arteries. These are the major arteries that supply blood to the brain, head and neck. This narrowing of the arteries is caused by a build-up of plaque. This plaque may cause turbulent blood flow and material breaking off can lodge in the brain, causing either transient symptoms or a stroke. Those with transient symptoms have the highest risk of stroke in the period immediately following the onset of symptoms.
The risk of stroke can be reduced if surgery is performed quickly following onset of symptoms. For patients with a narrowing of an artery between 50% and 99%, it is recommended that surgery to remove the plaque, a carotid endarterectomy, is performed within two weeks.
The status column indicates whether the surgeon had outcomes in the expected range given their level of activity ( ▲ ) or was found to be an outlier (X) in our assessment of their risk-adjusted outcomes.
Key to table column headings:
- Trust Name of the NHS trust
- Name of consultant surgeon
- GMC number of consultant surgeon
- AAA Total number of AAA repair procedures performed
- Open Number of open repair procedures performed
- EVAR Number of EVAR procedures performed
- Mortality Overall in-hospital mortality rate for that surgeon (unadjusted)
- Status Whether the surgeon mortality was within the expected range
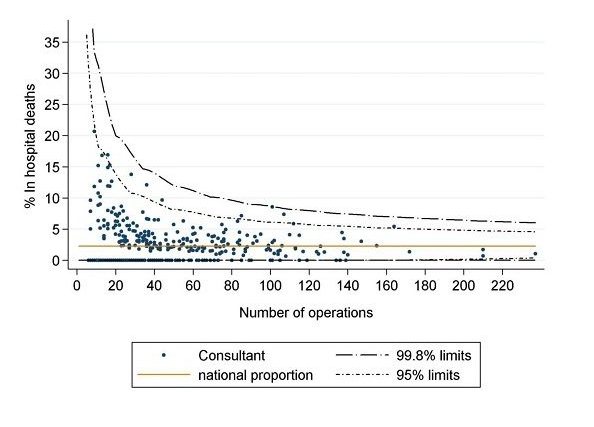
Funnel plot of risk-adjusted in-hospital mortality after elective AAA repair, with surgeon figures shown in comparison to the national average rate of 2.2%